

- The spine is the frequent site for metastasis
- Certain tumors have a unique manifestation in the vertebrae
- Malignant tumors most common in lumbar spine (lumbar > thoracic > cervical)
- Malignant tumors more commonly in vertebral body than posterior elements
Metastatic breast cancer

Metastasis
- Most common tumors of the spine
- Spread to vertebral body first, then later to pedicles
- Breast, lung, and prostate cancers are most common
Signs/Symptoms of Metastasis:
- History of cancer
- Recent unexplained weight loss
- Night pain
- Age > 50 years
Radiographic appearance of Metastasis:
- Most are osteolytic
- Prostate cancer is an osteoblastic tumor (osteoid forming tumor)
- Most not visible on plain radiographs until > 30% of vertebral body destruction
Treatment of Metastasis:
- Prognosis is poor if neurologic dysfunction, proximal lesions, long duration of symptoms, rapid growth of lesions
- CT-guided needle biopsy performed when possible, surgery avoided
- Radiation and Chemotherapy mainstays
- Prostate and lymphoid tumors are very radiosensitive
- Breast cancer is 70% radiosensitive, 30% resistant
- GI and renal cell tumors are usually radioresistant
Surgical indications:
- Progressive neurologic dysfunction unresponsive to radiation therapy
- Persistent pain despite radiation
- Need for diagnostic biopsy
- Pathologic fracture/dislocation
- Life expectancy should dictate whether or not surgical treatment is preformed
- For instability/neurologic deficit, anterior decompression and stabilization often used
Primary Tumors
- Tumors of the Vertebral Body:
- Eosinophilic Granuloma
- Usually seen in children Predilection for thoracic spine
- Causes progressive back pain
- Classically causes vertebral flattening, vertebra plana – Calve’s disease, seen on lateral radiograph
- Treatment:
- Chemotherapy for systemic histiocytosis
- Bracing to prevent progressive kyphosis
- Low-dose radiation may be indicated in presence of neurologic deficit
- Most symptoms are self-limited
- 50% reconstitution of vertebral height expected
- Giant Cell Tumor
- Most commonly seen in 4th-5th decade of life
- Expansile destruction of vertebral body
- Surgical excision and bone grafting recommended treatment
- High recurrence rate reported
- Radiation therapy should be avoided due to risk of malignant degeneration
Giant cell tumor of the L3 vertebral body

- Chordoma
- Low-grade lytic lesion in midline of sacrum or base of skull
- May occur in vertebrae
- Patients present with intra-abdominal complaints and pre-sacral mass
- Treatment: Radiation and Surgery
- Surgical excision may include unilateral resection of all sacral nerve roots
- Bowel and bladder function can be preserved by unilateral root resection
- High recurrence rates
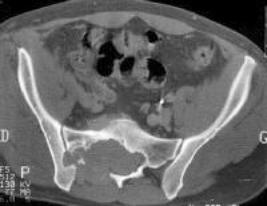
CT scan of sacrococcygeal chordoma
- Osteosarcoma
- Uncommon in spine (all primary malignant skeletal lesions)
- Poor prognosis
- Treatment: Radiation and chemotherapy
- Aggressive surgical excision occasionally performed
- Hemangioma
- Usually asymptomatic
- Small fractures may be present in symptomatic patients over age 40
- Radiographic appearance:
- “Jailhouse striations” seen on plain films
- “Spikes of bone” seen on CT
- Vertebrae normal sized, not expanded as in Paget’s
- Treatment
- Observation unless painful pathologic fracture present
- Anterior resection and fusion if posterior collapse
- Massive bleeding frequently encountered
- Marrow cell tumors: Multiple Myeloma & Plasmacytoma
- Common in spine
- Osteopenic, lytic lesions
- Pain, pathologic fractures and diffuse osteoprosis present
- Increased serum calcium levels
- Decrease hematocrit
- Abnormal protein studies (serum/urine electrophoresis)
- Treatment mainstay is radiation therapy (3000-4000 cGy +/- chemo)
- Surgery reserved for instability or refractory neurologic symptoms
Tumors of the Posterior Elements:
- Osteoblastoma and Osteoid osteoma
- Common in the spine
- May present as painful scoliosis in children – lesion is typically at apex of convexity
- Pain is typically relieved by non-steroidal anti-inflammatory drugs (NSAIDs)
- Bone scan helps localize
- Thin-cut CT scan directs surgical intervention
- Surgery indicated with scoliosis, curve resolves within 18 months of resection in children NSAIDs are mainstay of treatment if no scoliosis present
- Resection performed if pain uncontrolled by NSAIDs
- Osteoblastomas common in posterior elements of older patients
- Neurologic involvement in 50%
- Resection and posterior fusion typically required
Osteoid osteoma of L3 vertebra in patient 9 years of age with back pain and mild scoliosis. Sclerotic lesion is seen in pedicle of L3 on concave side of curve.
- Aneurysmal bone cyst
- Cysts typically detected during second decade of life
- May represent degeneration of more aggressive tumors
- Can occur in posterior or anterior elements (vertebral body)
- Treatment is excision and/or radiation therapy
Imaging:
- Plain radiographs
- Radiographic changes include absent pedicle, cortical erosion or expansion, and vertebral collapse
- MRI also useful: malignant tumors have decreased T1 and increased T2 intensity
- MR sensitivity increases with use of gadolinium
- Treatment:
- Complete resection is difficult
- Treatment usually comprises tumor debulking with stabilization
- Adjuvant chemotherapy and radiation are necessary