

Enchondroma is a benign tumor of bone that represents a hamartomatous process. Usually the lesions are asymptomatic and will present as an incidental finding or pathologic fracture. Fifty percent of these lesions will involve small tubular bones of the hands and feet, where pathologic fractures are common. There is no age, race, or gender predilection. The lesions tend to involve the metaphyseal regions of the proximal femur and humerus and distal femur. The hand is the exception in that it often involves the diaphysis.
Radiographically the lesions of the hands and feet are distinct from the lesions of the long bones. Lesions of the long bones are central and lytic with sharp margins, variable amounts of calcific stippling and no cortical involvement. On the contrary, lesions of the hands show marked cortical thinning and expansion with associated central calcific stippling (Figure #9,10). Absence of calcific stippling is not uncommon in active lesions. Histologically the lesions are also distinct. In the metaphyseal lesions of long bones there are found small numbers of cells within lacunae and no concerning features. Lesion of the hands and feet, however, show worrisome histological features and hypercellularity.
Figure #9

Enchondroma of the proximal phalanx.
www.orthoteers.co.uk
Figure # 10
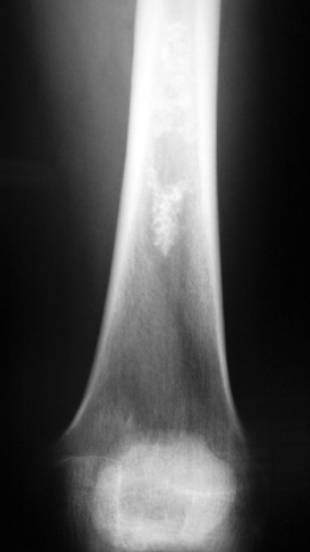
Enchondroma of the distal femur
www.sarcoma.org
Multiple enchondromatosis, or Ollier’s disease, describes the presence of multiple enchondromatous lesions throughout the metaphysis of multiple bones. It typically involves bones on a single side of the body and is capable of causing shortening and bowing of the affected regions while thinning the cortex dramatically. It is not infrequently confused with polystotic fibrous dysplasia. The presence of mutiple enchondromas and soft-tissue angiomas is known as Mafucci’s syndrome.
The risk of malignancy with these lesions is slight. There is less than 5% risk with an isolated lesion and solitary lesions of the hand are even less. Conversion to cancer occurs thru the process of dedifferentiation to chondrosarcoma. For the pathologist, this spectrum of disease is problematic and often a low-grade chondrosarcoma is indistinguishable from an enchondroma. In most cases, onset of new pain concurs with the dedifferentiation process. Ollier’s disease has an elevated risk at 20-30% risk of conversion and Maffucci’s has a near 100% conversion risk, making proper diagnosis and follow-up imperative. In addition, those with multiple enchondromatosis have an increased risk of visceral malignancies such as GI malignancies and astrocytomas.
Treatment of the incidental finding of a lesion is watchful waiting. If the lesion becomes symptomatic then curettage of the lesion with pathologic examination is warranted. Pathologic fractures of the fingers and toes are allowed to heal and then the lesions are curetted and bone grafted.