

Langerhans Cell Histiocytosis (LCH) has collected many pseudonyms over the years including histiocytosis X and eosinophilic granuloma (EG). It has twice the prevalence in male patients compared to females and strikes in the 5-15 year old range. Lesions are usually solitary but 10% will have two to three foci. It most commonly affects the skull but also carries a predilection for the spine. Symptoms are usually constitutional, such as fever, and patients often have symptoms of pain over the lesion. Labs are non-specific and often only present with an elevated ESR.
Radiographic studies show a lytic lesion that can affect any segment of bone beginning in the diaphysis and progressing to the epiphysis rarely. Over time, weakening of the vertebra in the spine will cause flattening of the vertebrae known as “vertebrae planae.” (Figure #12A, 12B, 13) The radiographic appearance can easily be mistaken for Ewing’s sarcoma, metastatic neuroblastoma, and osteomyelitis. Histologically these lesions show large histiocytes speckled with eosinophils (Figure #11). The eosinophils were once thought to be a primary determinate of the disease (thus the name eosinophilic granuloma), but are now thought to be secondary findings.
Figure # 11
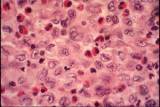
Langerhan’s cell histiocytosis. Note the eosinophils.
www.courses.ahc.umn.edu
Figure #12A

Figure 12A and 12B show AP and lateral radiographs of the lumbar spine with flattened L3 and L5 vertebrae.
www.medicine.cmu.ac
{kind=link}
Figure #12B

Figure #13
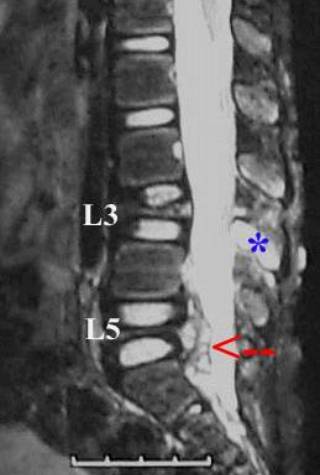
MRI of langerhan’s cell histiocytosis in the spine with vertebrae planae at L3 and L5 at the arrows.www.medicine.cmu.ac.th
Treatment of this disease is conservative and allows the disease to burn out. If the pain is unbearable, then curettage and steroid injection can be helpful. As a last resort, low-dose XRT for lesions in the spine or pelvis can also be helpful.
LCH has a peculiar association with Diabetes Insipidus that combine to create Hans-Christian-Schueller Disease that will show extreme thirst, polyuria, and vertebrae planae.