

The Aneurysmal Bone Cyst (ABC) is a benign tumor of bone found most commonly in female patients between 10 and 20 years of age. It has a predilection for the femur; though, also commonly found in the tibia, spine and pelvis. Two-thirds of spinal lesions will present in the posterior elements; a distinction it shares with osteoid osteoma, Giant Cell Tumor (GCT), and osteoblastoma.
Radiographically, it initially appears as an aggressive lytic lesion with permeative cortical destruction. It will progress to form a large aneurysmal bulge with a reactive cortical rim (Figure #3). Painful stress fractures in the thinned cortical bone are possible and usually account for the symptomatic presentation of these otherwise clinically silent lesions. Grossly they are filled with aged blood that has been termed to have the appearance of “crank-case oil.” Histologically, numerous blood lakes are the hallmark separated by fibrous septae (Figure #4). Giant cells are frequently encountered. The etiology is unknown but most think trauma is the likely inciting event with subsequent hemorrhage creating a hydraulic dynamic effect which progresses into an expanding hemorrhagic lesion. The natural progression of this lesion is spontaneous evolution, often preceded by trauma to the region (such as fracture). An involuted ABC will leave a thick rim of cortical bone easily identified radiographically.
Figure #3
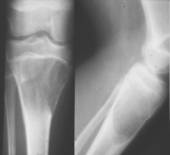
ABC of the proximal tibia.
myweb.lsbu.ac.uk
Figure #4
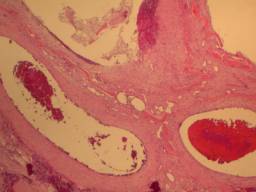
Low-power micrograph of an ABC. Note the multiple “blood lakes”
www.sarcoma.org
Therapeutic modalities are aimed at hastening the involution process. This most commonly includes intralesional curettage with bone grafting. Large, expanding lesions can often be reigned-in by embolization. Radiation therapy has been successfully used in the past but is no longer considered an option due to long-term carcinogenic risk. Prevention of pathologic fracture is imperative as the defects often leave little structural bone available for repair. This is particularly crucial in the peritrochanteric region and a course of limited weight bearing may be required.
The differential diagnosis of ABC includes: GCT, Solitary Bone Cyst (SBC), Ewing’s Sarcoma, telangectatic osteosarcoma, and chondromyxoid fibroma. Differentiating factors with GCT include the fact that GCT rarely present under the age of 20 and have twice the frequency of ABCs. In the spine, GCT often arise in the vertebral body; whereas, ABCs are more often in the posterior elements. ABCs can be nearly indistinguishable from other lesions, which necessitates timely biopsy of multiple regions to ensure a more malignant lesion is not the causative agent.