

The original principles developed by Sir John Charnley in the hip were translated to the knee by Gunston in the late 1960’s and published in JBJS in 1971. (35) From this beginning, in 1997, a total of 277,000 knee arthroplasties were performed, reflecting annual increases in the 1990s of more than 10%. (36) In addition, a recent article in JAMA concluded that knee replacement is an underused option when nonsurgical therapies fail. It is estimated that clinically significant osteoarthritis of the knee affects 5% to 10% of people over 60 years of age. It is clear that total knee arthroplasty (TKA) is one of the most successful and commonly performed orthopedic surgeries and is only going to be performed more commonly (Figure 34). This success is thanks in part to improvements in design, standardization of operative technique, infection prophylaxis, and new fixation techniques that have led to extremely low rates of revision.
Figure 34. Total hip and knee arthroplasty projections 1996 to 2030. From Future Demand for Orthopedic Skills to Soar. AAOS Bull 1999; 47:14. (36)

INDICATIONS
As with total hip indications, the indications for TKA continue to expand as advances in implant design and surgical technique improve patient outcomes. Early total knee designs were generally reserved for elderly, sedentary patients with debilitating pain and loss of function. The ability to predictably achieve excellent 10- to 15-year outcomes with TKA has encouraged many surgeons to consider performing TKA on younger patients who have increased activity requirements and performance expectations. ) After a diagnosis has been reached, the goals of intervention can be discussed with the patient. Then, after all conservative measures have been exhausted, operative planning should commence.
As discussed in the hip section, an essential prerequisite for total joint arthroplasty is significant joint pain, dysfunction, or both caused from intra-articular etiologies within the knee. Sclerotic and arthritic changes should be confirmed with radiographs to suggest that the knee joint is damaged sufficiently to explain the symptoms. Severe knee DJD is associated with knee instability from loose ligaments in the presence of a worn down loose interface. As with any elective surgery, the symptom severity necessary to justify arthroplasty must be weighed in light of the potential operative risks and benefits of a given patient. The more severe a patient’s pain and disability, the stronger the indication is. The more comorbidities a patient has, the more caution should be exercised. As with hips, most patients with pain that markedly limits ambulation, interferes with sleep, or requires narcotic pain medication are strong candidates for surgery. Patients with tri-compartmental (medial and lateral condyles plus the patellar femoral joint) disease are especially good candidates for TKA. Alternative procedures such as high tibial osteotomies (see below) and unicompartmental replacements can be used in very select patients. To address bone on bone patellar femoral joint arthritis, there is no good current solution other than TKA.
As with all joint replacement surgeries, considerations for conservative alternative treatments such as NSAIDS, cortico-steroid injections, canes and unloading braces and weight loss should be exhausted prior to undergoing total knee arthroplasty. As in the hip a vigilant pursuit of contraindications should be undertaken prior to undergoing surgery. (Figure 13)
Types of Implants
Kinematically, the native knee joint is more complicated than a simple “hinge” joint. Ideally, a TKA device should impart excellent range of motion, multiplanar stability, and maximal articular surface contact area. It should attempt to recreate the complicated sagittal and rotational kinematic motions that occur during flexion and extension of the normal knee. Solidly hinged and overly conforming TKA system increases the stability of a TKA by increasing its constraint. However, the torsional, coronal, and sagittal stresses that are normally shared by the surrounding soft tissue structures are more fully transferred through to the bone-cement or bone-implant fixation interface, which can result in premature failure from aseptic loosening. (42-43) The failure of early TKA designs was due predominantly to premature aseptic loosening associated with malalignment, ligamentous instability, and especially the use of excessively constrained simple hinge-like implant devices. However, in the normal knee, there is a complicated pattern of motion that occurs between the femoral and tibial articular surfaces during flexion and extension which is not on a fixed transverse axis of rotation like a simple hinge, but rather about a constantly changing center of rotation (polycentric rotation). Motion is achieved by a complex coupled mechanism in which the femoral condyles simultaneously glide and roll back on the tibial plateaus about multiple simultaneous axes. This femoral rollback and is a predictable and controlled posterior rollback of the femoral condyles on the tibial plateau during flexion of the intact knee. (Figure 36-37) Roll back is due impart to the stabilizing nature of the relatively immobile medial meniscus, PCL, ACL and various other ligamentous structures on top of a very low friction articular surface. Roll back increases posterior clearance by putting the tibia further out in front of the femur, permitting greater flexion with out impingement and increases the moment arm of quadriceps by 20 to 30%. Interestingly, the rollback on the lateral side is more than the medial side averaging (14.1-19.2mm laterally while the medial condyle translates posteriorly less than 5 mm). Therefore, there is external rotation of the femur on the tibia during flexion and internal rotation during extension. (ie, screw home mechanism) adding another axis of rotation to the knee. Rollback also increases the length of quadriceps moment-arm. If femoral roll back is not designed in prosthetic knee, effective strength of quadriceps is reduced by about 30%.
Figure 36
Knee motion is known not to function as a simple hinge but to involve an extremely complex series of movements about variable axes and in three separate planes. Flexion and extension do not occur about a fixed transverse axis of rotation but rather about a constantly changing center of rotation (polycentric rotation). Motion is therefore achieved by a complex coupled mechanism in which the femoral condyles simultaneously glide and roll back on the tibial plateaus. In addition to flexion and extension, concurrent axial rotation also occurs.
Figure 37
Actual knee motion involves both sliding and rolling, as shown above in part C.
Both PCL retaining and PCL sacrificing (AKA posterior/semi constrained prosthesis and PCL-substituting) implants are used. The eccentric femoral origin of the PCL produces a tensile force in the ligament as the knee flexes that is converted into a translatory force, shifting tibia forward or forcing femur to “roll back.” Retention of the PCL theoretically increases flexion with normal rollback but requires that the slope of replaced femoral condyles closely match that of the native condyles and that the knee be well balanced. The initial unconstrained implant designs that sacrificed both the PCL and ACL did not allow for rollback with a maximum flexion of 95º. These designs also had significant flexion instability. Preserving the PCL mitigates against flexion instability and cause rollback even without the ACL. However, this ACL deficient rollback is a combination roll and slide that can cause increased poly wear. This rollback also requires polyethylene to be relatively flat with less conformity on the femoral condyles. This effectively concentrates contact forces and can lead to rapid poly wear. Newer PCL retaining implants have a more congruent polyethylene that allows for less rollback but also spreads out contact forces leading to less poly wear. However, overly constrained implants can cause aseptic loosening because of excess stress transferred to the implant/cement/bone interfaces. TKA designs can reduce loosening by lessening stresses generated at the fixation interfaces but at the expense of accelerated polyethylene wear from increase peak pressures at the joint surface. The newest designs have developed an excellent balance between excessive stress transfer to the fixation site from over conformity and excessive poly wear from high contact pressures. The polyethylene inserts are “dished” in appearance in both the coronal and sagittal planes. Improvements in surgical instrumentation and techniques (ligamentous balancing, etc) have resulted in dramatic reduction in implant loosening as these problems were better addressed. The current goals of TKA design focus on minimizing polyethylene wear while protecting the integrity of the fixation interface.
TKA designs that remove the PCL may have less of a flexion arc and produce a quadriceps force which is weaker.
Theoretically, in semiconstrained components where the sagittal radius of the femoral component is constant though out, knee flexion would be expected to be limited to 120º with less roll back in flexion than a PCL retention device. Newer PCL sacrificing devices provide AP stability with an intercondylar spine or post built into the polyethylene and articulates with the transverse cam situated between the femoral condyles. This device mimics the kinematics of the PCL and augments flexion. The disadvantage of this device is that if the flexion gap is not balanced and is too large, a “cam jump” can occur, effectively dislocating the tibial post and tibia anterior to the femur. This must be reduced expeditiously and often requires a general anesthetic to do so. Cam jump can occur in the hyper-flexed knee even with careful balancing and therefore patients with expected knee motion > 130 º flexion should consider a PCL retaining implant.
Careful balancing of flexion extension gaps is important in both type of prosthesis but might be made more difficult in a PCL retaining knee where exposure is more limited. Newer semi-constrained knees that sacrifice the PCL avoid many problems of superfluous constraint while mimicking the function of the PCL. Excellent results from both types of prosthesis are possible. Gait analysis comparisons while level walking did not show any significant difference between retaining or removing PCL. However, patients without a PCL shift their weight farther forward with each step while climbing stairs. This is thought to be due in part from excess leaning forward while stair climbing with a shortened quadriceps mechanism lever arm and less roll back provided by the PCL. A recent report comparing functional outcome between matched pairs cruciate retention and posterior stabilized knees showed no statistically significant functional difference between the two groups in the clinical evaluations. (44) There is no definitive answer as to weather PCL retaining or sacrificing knees provide a superior construct but there is a trend toward PCL sacrificing knees.
Despite the fact that there is little difference in clinical results between well placed PCL retaining and sacrificing knees, the theoretical advantages of each design continues to drive research and innovation. The overall theoretical advantages and disadvantages of PCL retention are outlined below.
– Advantages of PCL retention:
– maintenance of ligament’s proprioceptive abilities;
– maintenance of load transfers by the PCL;
– allows stress sharing, so that stress is taken on bone cement interface;
– Can provide increased rollback and therefore better flexion and should be considered for patients that
are expected to require >130 degrees of flexion.
– AP stability enhanced although many semi-constrained implants have good AP stability as well.
– Retention of PCL results in more normal gait pattern during stair climbing, partly because of the
ability to maintain normal flexion moment of knee during stair climbing
-Less risk of synovial entrapment and patellar clunk syndrome
– Disadvantages:
-Adequate exposure of proximal tibia can be difficult w/ PCL retention
-Can be difficult to balance collateral ligaments with varus/valgus deformities while preserving the PCL
-Significant proximal tibial resection may jeopardize the PCL insertion, in which case a posterior
stabilized prosthesis will be required; this is especially true in malpositioning of the joint line where significant
proximal tiabl resection can be required.
-Revision TKA will require sacrificing PCL
-Rheumatoid knees often do not have enough strength and resilience in their nacent PCL to support the
Prosthesis and will often stretch or loosen
-Patients with prior trauma to the PCL are not good candidates for this device
-Patients with a previous patellectomy require a PCL- substituting implant because the weaker extensor
force allows for easier anterior dislocation even if the PCL is intact.
-Excessive posterior roll back can be seen with PCL retention when the PCL is too tight.
-If tightness remains on medial side despite release of medial collateral ligaments & posterior capsule a PCL
sacrificing prosthesis is indicated in order to release the PCL
-PCL retention can increase polyethylene wear from sliding during rollback unless careful balancing is obtained
with newer more conformed implants.
Fixation in the knee, as in the hip, is accomplished with both cemented and uncemented techniques. There is significant controversy surrounding which type of device provides optimum fixation. In brief, many surgeons favor noncemented knees in younger active patients where the biological remodeling potential exists at the bone prosthetic interface to re-anneal any microfracture incurred during vigorous activity. Micro-fractures at the bone prosthetic or bone cement interface can result in loosening, but press fit knees can theoretically heal these small breaks with biologic “spot welds”. This theoretically provides for better long term implant survival in such patients. However, other surgeons prefer cemented fixation especially in elderly osteoporotic, rheumatoid patients, or patients subjected to prior irradiation who have little biologic potential for ingrowth. Such patients might precociously loosen with early failure because the never developed sufficient biologic fixation in the first place. This reasoning is supported by the well established fact that uncemented press fit acetabular components fail with aseptic loosening at a significantly higher rate than cemented components in patient treated with irradiation to the pelvis. These surgeons also argue that cemented implants provide immediate fixation allowing for earlier safer weight bearing and are less expensive than the newer press fit knees. Interestingly, one randomized controlled trial of cemented versus cementless press-fit condylar total knee replacements in 501 replacements showed a ten-year survival of 95.3% and 95.6% in the cemented and cementless groups, respectively. (39) Another study reported a higher revision rate in press fit knees but similar function and outcomes scores. (40) Nevertheless, these similar results will only assure that the debate will continue for the time being in the knee.
Backside polyethylene wear is wear on the inferior surface of the tibial polyethylene inserts. It is a significant source of microscopic polyethylene particles and osteolysis. Backside wear is a result of inadequate locking mechanisms. It has been estimated that the amount of debris released from this pseudo-backside articulation may be 2-100 times greater than the debris generated at the femorotibial articulation. Newer TKA designs have improved insert locking mechanisms and as a result generate significantly less poly wear.
The use of gamma irradiation sterilization techniques in the presence of oxygen has been shown to cause accelerated polyethylene wear due to increased oxidation of polyethylene and disruption of polyethylene polymer chain. s due to oxidative chain scission. Newer sterilization techniques reduce the rate of polyethylene oxidation and thus reduce associated polyethylene degradation and wear. Ethylene oxide gas sterilization is a better technique, but still is associated with significant wear. Poly sterilization with gamma irradiation in an inert environment (inert gas or vacuum) has been shown to preserve the best wear characteristics of the polyethelene. Knee simulator data suggests that poly wear can be reduced as much as 50% using these techniques. (45)
Figure 38
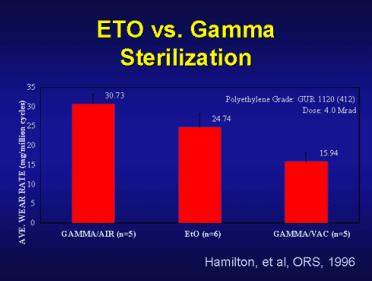
Figure 3 Figure 38. Graph demonstrates average polyethylene wear rates (mg/million cycles) when comparing sterilization techniques using gamma irradiation in air vs ethylene oxide vs gamma irradiation in an inert vacuum environment.
The thickness of the polyethylene is important to prevent catastrophic failure. Polyethylene thickness must be at least 8 mm to keep the yield strength of the ultrahigh molecular weight polyethylene above the contact stresses experienced in the typical TKA. In larger patients, or patients that are young and more physically active larger polyethylene implants should be considered and accounted for when balancing the knee. Obviously the thinner the poly insert the smaller its yield strength and the critical cutoff is about 8-10mm of thickness.
In summary design factors shown in various analyses to reduce polyethylene wear include: use of thicker polyethylene bearings, reducing backside wear by improving locking mechanisms of modular tibial polyethylene components, use of better sterilization techniques (of gamma irradiation sterilization techniques in a vacuum without the presence of oxygen, use of TKA designs with increased articular surface conformity, and the use of mobile bearing TKA systems. Both PCL substituting and PCL retaining implants can produce excellent results but both have patient specific considerations that should be made prior to surgery.
Preoperative Evaluation
As discussed in the hip section, it is crucial to establish the etiology of knee symptoms prior to embarking on a surgical remedy. Examination of the knee begins in the hip. Frequently patients will present with the chief complaint of knee pain when they have little evidence of DJD in their knees but have profound joint disease in their hips or lumbar spine. The hip and lumbar spine must be evaluated with every knee examination. As discussed previously they share innervation (obtorator nerve {L2,3,4}} which accounts for the referred pain phenomena. In addition to a full past medical history prior history of trauma, infection, or neoplasia to the affected joint should be evaluated. As with any orthopaedic examination, first active and then passive range of motion should be assessed and documented. Patient’s strength in their available range as well as their gait should also be evaluated. It should be noted that normal gait requires 67 degrees of flexion in the swing phase, 83 degrees of flexion for stair climbing, 90 degrees of flexion for descending stairs, and 93 degrees of flexion in rising from a chair.
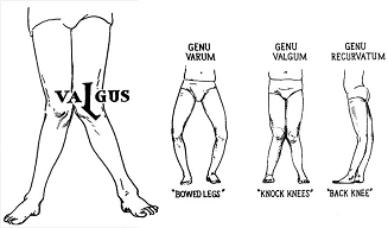
Intra-articular knee pain may originate from either femoral condyle of the tibio-femoral joint or the patellar femoral joint. Patients with significant knee DJD will often report instability or their knee or “giving way” from ligamentous insufficiency from a worn down loose interface. Tibio-femoral condyle DJD is often associated with degenerative meniscal tears most commonly on the medial side. Either or both femoral condyles can be affected but the most common pattern is medial tibio-femoral joint disease with an associated varus deformity. Mechanical symptoms such as locking or clicking while bending or twisting is often associated with meniscal tears. Medial joint line pain with deep flexion is most commonly from a medial meniscus tear. Degenerative tears of the medial meniscus are the most common form of meniscal tears and are commonly concurrently present with significant articular cartilage wear. Some younger patients(50-60’s) with OA that experience acute onset of mechanical symptoms are candidates for arthroscopic meniscectomy. This maneuver might be able to “by some time” or post pone there need of TKR for a latter time when revision surgery of their index TKR would be less likely. In patients with OA, intra-articular injections with bupivacaine and depomedrol are not only therapeutic but diagnostic as pain relief signals intra-articular pathology regardless of the etiology. Varus and valgus deformities Figure 35 (varus= distal limb pointing toward the midline [bow-legged], valgus= distal limb pointing away from midline[nock knee]), also known as coronal plane deformities should be assed preoperatively to plan appropriate correction. Occasionally, young patients with only medial compartment disease and associated varus deformity with no patellar or lateral compartment involvement may be candidates for high tibial osteotomies (see below). These procedures often will “buy the patient time” before having to commit to TKA. Sagittal plane deformities such as flexion and extension contractures and or procurvatum and recurvatum should also be assessed. Patellar femoral pain is often elicited by walking up and down stairs or hills. There will frequently be crepitance on exam in the affected knee. Often times the patella is the most severely affected part of the knee. Despite ongoing research on isolated patellar resurfacing, the treatment for isolated end-stage patellar femoral joint disease today is a total knee arthroplasty.
Figure 35 Demonstrates valgus, varus, and recurvatum deformities of the knee joint.
While examining the patient it is important to note any previous incisions, limb length discrepancy, hip and foot deformity. Inability to flex the ipsilateral hip, such as with a hip fusion, can make operative positioning difficult during TKA. Rheumatoid arthritis patients often suffer from concomitant arthritis of both the hip and knee. Generally, hip arthroplasty should be performed prior to knee arthroplasty, because hip flexion is needed while performing a TKA, and the hip is more tolerant of delayed rehabilitation than the knee is. A valgus foot puts a valgus strain upon the knee. Considering correction of ankle deformity prior to TKR is advisable. If operative correction of the ankle is not done, then standard tibio-femoral cuts could leave the ankle with a severe valgus deformity. In rheumatoid patients, a deformity of the foot may be the main cause of the deformity of knee. A patients vascular status should be carefully evaluated prior to proceeding. If a patient does not have palpable pulses distally with good doppler signals, then the surgeon should consider not using a tourniquet during the case to avoid vascular embarrassment. Additionally, if the patient has diabetes with pulses that are not palpable but are dopplerable or the patient is a non-diabetic without doppler signals, then a vascular surgery consult should be obtained to explore options for augmenting perfusion. (46)
Complete preoperative radiographs to evaluate the knee include: 1)Standing full length AP film from the hip to ankle, this film allows for evaluation of mechanical axis of the entire lower extremity as well as evaluating for prior trauma or neoplastic lesions in the adjacent areas. 2) Standing extension lateral on large cassette (14” X 17”) 3) Flexion AP and lateral on large cassettes to evaluate the posterior aspect of tibio-femoral joint as well as sagital plane deformity. Flexion films will often reveal a more extensive pattern of DJD and joint space narrowing than is shown on the extension films of the knee. 4) Merchant’s or sunrise views to evaluate the patellar-femoral joint. Preoperative radiographs reveal the patients current mechanical axis and alert the surgeon as to the possibility of needing to perform soft tissue releases to balance the knee after bony cuts have been made in an anatomic fashion. Normal mechanics of the lower extremity have the tibia in slight valgus (3 degrees) relative to the femur with the tibial mechanical and anatomic axis being coincident. Figure 36. The aims of TKA include restoring the normal mechanical axis of the leg while balancing the soft tissue of the knee to optimize its biomechanics. Plain films are invaluable in achieving these goals and are required for completing device specific templating of the knee to in accomplishing these goals.
Figure 36: Demonstrates mechanical (line from the center of the femoral head to the center of the distal tibia) and anatomical axis (line down the shaft of the respective long bone) of the lower extremity and their relationship to the vertical axis. Note the mechanical and anatomic axes of the tibia are coincident and that the femoral anatomic axis is 6º valgus to the femoral mechanical axis in the normal lower extremity. Varus and valgus mechanical axes are also drawn. Normal mechanical axes pass through the central third of the knee.

Because arthroplasty often is associated with significant blood loss, options for autologous blood donation prior to surgery should be discussed with the patient preoperatively. Recently, the use of a cell saver device intra-operatively and postoperatively via surgical drain collection has been shown to significantly reduce the need for transfusion as well as being cost effective.(38)
Surgical Technique
Several exposures have been adapted to TKR. The most commonly used approach in TKA is the medial parapatellar approach. Figure 37. This exposure is started with a longitudinal midline or medial parapatellar skin incision. It is important to keep in mind that the superficial blood supply comes mainly from the medial side of the knee and this approach will leave the patient with some numb spots on the lateral aspect of the knee. Additionally, in revision surgery where a much larger exposure is required, a more lateral incision should be used to not “outflank” the blood supply to the skin flaps above. During deep dissection an arthrotomy is made on the medial side if the patella leaving approximately 2-3mm of retinacular tissue to close the joint with. This arthrotomy is carried proximally and distally in the tendonous tissue until the patella can be everted laterally. It is important to avoid dissecting into the vastus medialis as well as leaving enough tendounous tissue to sew on both sides of the arthrotomy. Scissors can be used to transect the patellafemoral ligament off the femur and a synovectomy is performed at this point (if appropriate). Some surgeons trim the anterior fat pad but do not remove it entirely to provide extra vasculature and padding to the surrounding soft tissues. Patellar resurfacing can be performed early in the exposure in order to thin the patella and facilitate the eversion. After the patella is everted and the knee flexed the tibial insertion of the ACL can be incised which allows the tibial to be subluxated forward to allow complete visualization of the plateau surfaces. A rongeur is used to remove marginal osteophytes from the femoral condyles, patella and tibia as well and intercondylar space. Osteophytes from intercondylar notch of femur should be removed particularly if prosthesis is designed to retain PCL as the may abrade and impinge on the PCL. A lateral parapatellar approach is sometimes used in very valgus knees where there will be significant resection off of the medial femoral condyle. It is also occasionally employed for difficult primary /revision knee replacement, to protect the tibial tubercle from avulsing on lateral rotation of the patella.
Figure 37 Medial parapatellar, approach to the knee.

A subvastus approach is commonly used approach with a medial parapatellar like incision. This approach spears dissection of the vastus medialis. (Figure 38) The Vastus medialis is reflected laterally as deep dissection veers medially through the retinacullum at the shoulder of the patella. Advocates of this approach report less interference with the extensor mechanism. However, in very obese patients it is often difficult to obtain a good view with this approach.
Figure 38.
During revision surgery when significantly larger exposure is needed a rectus snip (Figure 39) or Quadriceps turndown (figure 40) can be used to expand the standard medial parapatellar exposure.Care should be taken to avoid the lateral superior genicular artery especially with the quadriceps turndown. The quad turndown can be converted into a Y on closure if there has been quads contraction secondary to knee stiffness. It is important not to repair the with a flexion contracture. Therefore the arthrotomy should be stitched in the position where gravity alone will allow flexion to 90 degrees Post operatively active extension should be delayed and a splint used for walking for 2-3 months.
Figure 39
Figure 40
After obtaining adequate exposure bone preparation and ligamentous balancing can begin. The key surgeon-controlled details crucial to restoring an anatomic articular surface are 1) reproduction of anatomic extremity alignment, 2)restoration of the proper joint-line level, and 3)assurance of symmetry and balance of the flexion and extension gaps.
During proximal tibial resection the remnant menisci are sharply removed. Care should be taken to avoid the potential of vascular injury. The popliteal artery lies behind the posterior horn of the lateral meniscus, and will be partially protected by the popliteus mucle. The popliteal vein lies directly posterior to the PCL. The menisci are removed by pulling them into the joint and transecting them with a knife blade or bovie tip directed parallel to posterior tibial surface. After tibial resection, it is important to rotate the tibial component optimally with the center 1/3 of the component line up with the tibial tubercle.
The distal femoral cut is usually the first to be made and it is done in 5-7 degrees of valgus from the anatomical axis of the femur (ie perpendicular to the mechanical axis of the limb). Most implants use an intramedullary alignment jig to assure precision. During femoral preparation the distal femoral cuts are established with an intramedullary guide. The starting canal entry point for the IM guide is 1cm above the insertion of the PCL and slightly medial to the midpoint of the intercondylar notch. This assures that the guide will be placed in the center of the femoral canal in line with its anatomical axis. Once the femoral guide is inserted and the varus valgus guide set (usually 6º valgus), 9-10mm of distal femur is resected which should be equivalent to the amount of bone to be replaced by the implant. It is important that this amount of bone taken off be equivalent to the thickness of the femoral component and polyethylene in order to recreate the original joint line and provide for a well balanced joint. The same is true of the tibial cuts to ensure a well balanced knee.
The second cuts to be made are the anterior and posterior femoral cuts, which remove the femoral trochlea and the posterior femoral condyles. To facilitate in balancing the knee and to enable normal central patellofemoral tracking, the flexion gap should be made rectangular. (Figure 41) The femoral cutting block on the femur should be placed in 3º of external rotation in relation to the posterior condyles. This is because the tibial cut will be perpendicular to the mechanical axis of the leg while the nascent tibial articular surface has a slightly elevated lateral plateau. Since the tibia will be made perpendicular, something needs to make up for this slightly higher lateral plateau. This 3º of external rotation cut into the femur when the knee is flexed makes up for the 3º difference at the plateaus and assures congruence between the anatomic axis of the femur and tibia. Additionally, if the femur is internally rotated instead of externally, the patella will subluxate laterally. A useful landmark for this cut is Whiteside’s line which perpendicular to the vertical line in the deepest part of the femoral trochlea /notch. This line is also perfectly perpendicular to the epicondylar axis or a line drawn between the medial and lateral epicondyles.
Figure 41
The femoral cut should be sized correctly to avoid notching of the anterior cortex of the femur. A well done anterior femoral cut is said to look like a baby grand piano. As mentioned above, the tibial cut should be made perpendicular to the mechanical axis of the limb. A posterior slope of 0-5 degrees is often incorporated to aid with deep flexion, depending on the design of prosthesis. However, many implants have no posterior slope so the flexion extension cuts are made perfectly perpendicular facilitating placement and balancing without compromising motion. Chamfer cuts on the femur are then made using the cutting jig. After the first femoral and tibial cuts are made, attention can be turned to balancing. Some systems allow for balancing with solid spacer blocks prior to making Chamfer cuts. The surgeon can use laminar spreaders to measure flexion/ extension gaps if no trial blocks are available for balancing prior to committing to Chamfer cuts. Balancing the flexion/ extension gap is to TKA as assessing hip stability with leg lengths, offset, and component design is to THA. A properly balanced knee is essential to achieve full range of motion. Additionally, proper attention to detail will ensure a more uniform loading of the articular surface and reduce polyethylene wear. The flexion gap is assessed with the knee in 90 degrees of flexion while the extension gap is best assessed with the knee in full extension. The flexion and extension gaps should be roughly equal to each other and rectangular. The solutions to making the flexion gap and extension gap equal and rectangular are well described in the table below. (Figure 42) In general, if the knee is tight in extension resect more distal femur and if it is tight in flexion cut more posterior femoral condyle. If the knee is tight in both, resect more tibia since this affects flexion and extension equally. Soft tissue balancing in the coronal plane should be performed after bony cuts and is discussed below.
Most bone loss in valgus deformities is femoral rather than tibial. When addressing these deformities it is important to be careful not to internally rotate the femoral component. To avoid this, the worn lateral condyle can be built up before fixing jig for the anterior and posterior cuts. No greater than a 5 degree femoral cut should be made. The surgeon can also consider lateral parapatellar approach in valgus knees. The final product should achieve full extension and > 120º flexion. It should be completely stable to varus/valgus stressing in full extension with slight laxity to varus/valgus stress in 20º of flexion. This demonstrates a knee very likely to have smooth easy motion and support the functional demands of the patient.
Figure 42: To make the flexion and extension gaps equal: This chart is money! It should be committed to memory. (Taken from Orthoteers.co.uk)
| FLEXION GAP LOOSE | FLEXION GAP OK | FLEXION GAP TIGHT | |
| EXTENSION GAP LOOSE | Potential problem-unstable knee
Solution- thicker plastic insert |
Potential problem- unstable in extension
Solution- 1.augment femur distally, or 2. downsize femur (cut off more posteriorly) to increase flexion gap, then use a thicker plastic insert |
Potential problem- unstable in extension, restricted flexion
Solution- Downsize femur to increase flexion gap, then use thicker plastic insert |
| EXTENSION GAP OK | Potential problem- unstable in flexion
Solution- resect more from distal femur to increase extension gap then use thicker plastic insert |
You are a dope surgeon | Potential problem-
Restricted flexion
Solution- Downsize femur to increase flexion gap Slope tibia more posteriorly to increase flexion gap |
| EXTENSION GAP TIGHT | Potential problem- Limited extension, unstable in flexion
Solution- 1.Resect distal femur to increase extension gap, thicker plastic insert 2. Release capsule posteriorly, thicker plastic |
Potential problem-
Limited extension
Solution- 1.Resect distal femur to increase extension gap 2. Release capsule posteriorly |
Potential problem-
Restriction of flexion and extension Solution- Thinner plastic insert but not less than 10mm Resect tibia which increases the flexion and extension gap equally |
Creating an elevated joint line is a problem that can occur during balancing the knee. It is defined as an increase in the vertical distance from the original articular surface to the newly reconstructed surface. Raising the joint line also creates an effective patella baja. Elevated joint lines often occur when the femoral component is under sized leading to a larger flexion gap than extension gap. To balance this, more bone is removed from the distal femur elevating the joint line. Also excessive medial or lateral releases and insertion of thicker plastic bushing can elevate the joint line. Preserving the joint line is important because it can affect the function of the PCL (in PCL preserving implants), collateral ligament function, and patellafemoral mechanics
In posterior stabilized implants a box cut is made on the distal femur. The box cutting jig should be placed flush on anterior and distal femoral surfaces centered over the intercondylar notch (or IM drill hole). If the knee has a valgus deformity consider slightly lateralizing the jig. It is essential that the box cuts not be medialized in relation to the intercondylar notch. This will force a corresponding medialization of the tibial component (resulting in increased Q angle and possible patellar subluxation). The surgeon should also be aware that many TKR systems use a box cut that is the same size regardless of the size of the distal femoral condyles. Therefore, in small and medium sizes the smaller lateral condyle is at risk for fracture if careless or rough technique is used while performing the box cut and broaching.
The most common complications in total knee arthroplasty affect patellafemoral tracking. Any factor that causes an increase in the Q angle can cause lateral mal-tracking of the patella. Internal rotation of the tibial component lateralizes the tibial tubercle thereby increasing the Q angle and inducing patella mal-tracking. This is another reason to error in slight external rotation if one cannot get the femoral component exactly rotated 3degrees externally. Medial translation of the femoral component causes the trochlea to be more medial increasing the Q angle. If the patella is resurfaced, the prosthetic patella should be medialized not just placed in the middle of the available bone to assure smooth tracking. An oversized femoral component can cause increased anterior displacement of the patella during knee motion leading to patellar instability and/or limited flexion. A nice test to remember intraoperatively to check patellar tracking is the “no thumb test”. Patella tracking is evaluated throughout full range of movement of the knee “without thumbs” on the patella. If the patella stays in the groove then tracking is adequate. If it laterally subluxates, the knee should be inspected for the above problems. If none of the above problems are present, perform a lateral retinacular release. The surgeon should consider not resurfacing the patella in the first place if less than 12mm of native bone remains. In such circumstances, patellar fracture and early loosening are common.
After the bony cuts have been completed, ligamentous balancing should be evaluated. Coronal plane (varus/valgus) deformity should be evaluated in both flexion and extension. The basic principle for both of these coronal plane deformities is to release the concave side of the deformity and thereby filling up the convex side until the ligaments are taught. Varus deformity of the knee is the most common deformity of the osteoarthritic knee. If there is still a residual varus deformity after bone resection, a medial release should be performed. This can be accomplished in the following order, but should be stopped as soon as the deformity is corrected. The ligamentous structures can be “pie crusted” prior to definitive resection. The following maneuvers should be utilized to balance a varus deformity.
- Removal of medial femoral and tibial osteophytes
- Release posteromedial capsule
- Release of deep medial collateral ligaments off the tibia at the posteromedial corner of the knee
- Release of the attachment of semimembranosis aponeurosis
- Release of the pes anserinus insertions in continuity with the periosteum
- If greater degree of deformity, may release PCL. Use caution when doing this as the popliteal vein lies directly behind the PCL. Valgus deformities are also common. They are found in rheumatoid arthritis from stretching of the medial capsule and ligaments. A valgus knee is seen in OA with hypoplasia of the lateral femoral condyle and commonly an associated flexion or external rotation contracture. The order of lateral releases can be remembered by the pneumonic [OCLIPLIPS]:
- Osteophytes removal
- Capsule (lateral) released from tibia
- Lateral patellafemoral ligament ( a distinct part of the retinaculum)
- Iliotibial band at level of joint (IT band release is better if the knee is tight in extension with a Z-type release off of Gerdy’s tubercle)
- Popliteus (Better when the valgus knee is tight in flexion and is often accomplished with a pie crusting technique)
- Lateral / Fibular collateral ligament from the femur (Release the LCL very judiciously as this causes the knee to be very lax and a posterior constrained implant should be used)
- Intermuscular septum
- PCL as it can act as a central tether
- BicepS tendon off fibula head
- If associated with a flexion contracture, posterolateral capsule and lateral head of gastrocnemius should be released from the femur
- Occasionally the medial collateral ligament is so attenuated that balance cannot be achieved The options available then are
- MCL advancement
- Constrained knee replacement in the elderly
- Varus/valgus constrained (VVC prosthesis)
Most of the sagittal plane balancing is done with a combination of bony cuts and ligamentous releases as described in Figure 42. When there is a preoperative flexion/extension contracture special considerations should be maid during this step. It is important to document the full pre-operative flexion and extension range of motion. The single most important factor governing ultimate flexion range after TKA is preoperative flexion range. If no further operative accommodations are made the prosthetic knee will never achieve better range than what the preoperative range was. As a general rule postoperative flexion range is equal to the preoperative flexion range +/- 10º unless surgical intervention is made. In the case of a flexion contracture, in addition to bony cuts listed in figure 42 the following maneuvers can be employed:
- Strip adherent posterior capsule from the femur after the femoral cuts made
- Removal of posterior osteophytes with a curved osteotome
- Division of PCL in constrained implants
- Release the tendinous origins of the gastrocnemius
- Another alternative is to remove more distal femur but this raises the joint line and the function of the collaterals if its excessive
Flexion contractures must be corrected at surgery because fixed flexion contractures will not stretch out. On the other hand flexion contractures that are seen postoperatively when there has been a surgical correction are often due to relative hamstring tightness and spasm. After the anterior arthrotomy the quadriceps will not fire vigorously leaving the knee with a relative over pull of the hamstrings. Normally, as knee swelling subsides, quad strength returns and almost all hamstring over pull will resolve by 6 months with continued improvement seen throughout the first year postoperatively. If 90º of flexion is not obtained by 6 weeks however there is likely some intra-articular block to flexion from arthrofibrosis and knee manipulation under anesthesia is warranted. Post-operative CPM (continuous passive motion) use and physical therapy are an essential component to full patient recovery.
Revision TKA
As the number of primary TKA increases the need for revision TKA also rises concurrently. Despite multiple advancements in implant design and surgical technique the major goals of revision knee surgery remain: a) Extraction of failed components with minimal soft tissue destruction b) restoration of cavitary and segmental bone defects c) Restoration of the original joint line as best as possible d) Balanced knee ligaments with good range of motion and e)stable fixation of new components.
Aseptic failure after TKR is caused by multiple factors. These include: component loosening, osteolysis from polywear (polyethylene particles are recognized by macrophages as foreign bodies initiating an immune response causing bone resorption and osteolysis), ligament instability, and patellafemoral maltracking. Tibial component loosening is more common than femoral component loosening. Many failed aseptic prosthetics are associated with a significant loss of bone stock which should guide the preoperative planning process and selection of revision prosthesis. The choice of revision implant also depends on the integrity of the MCL and PCL. If the knee is PCL deficient, or if the joint line is significantly altered, than a posterior stabilized is recommended. This type of implant should always be available in revision surgery, even if a PCL retaining system is planned because the integrity of the PCL is unpredictable. If the MCL is attenuated than a constrained non-hinged implant is recommended. Furthermore, if the MCL is completely incompetent, than a constrained hinged knee on a rotating platform is recommended.
Septic arthritis post TKR is also a common indication for revision surgery and is a potentially devastating complication. Prosthetic infections can be divided into three categories: a) early (within 4 weeks post operatively) b) hematogenous (outside nidus like an abscessed tooth seeds the implant; if the infection persists longer than 4 weeks it is equivalent to a late infection) and c) late infections(present for more than 4 weeks). With early post-op infections, most bacteria have not formed a glycocalyx on the implant. Therefore, prior to 4 weeks an infected prosthetic can be I&D’d with modular component and poly exchange followed by 6 weeks of targeted IV antibiosis. After four weeks, a two staged re-implantation should be undertaken. Such patients will have deep seeded infections that will not be eradicated with I&D alone. There is no chemical that can safely be used to remove the polysaccharide glycocalyx. In the first stage, infected components are removed, intraoperative cultures taken, and an antibiotic spacer is placed. An interval of 6 weeks of targeted IV antibiosis should follow after which definitive reconstruction can take place with permanent revision components. The interval of 6 weeks is assuming a benign ESR, WBC count, CRP and clinical presentation.
The condition of the local wound is paramount in determining the type of definitive reconstruction to be performed after infected components are removed. If soft tissue coverage deficits are present than local muscle rotational flaps can be used to allow for a tension free closure. In the case of the knee a gastrocnemius rotational flap could be used. Patients that have significant destruction and attenuation of ligament/musculotendonous complexes, will have an anticipated poor functioning prosthesis. Such patients should be considered for an arthrodesis (fusion). Amputation is reserved for patients who are extremely ill or who have severe soft tissue destruction, where neither reconstruction nor fusion will allow for adequate soft tissue coverage or provide a functional limb.
Bone deficits are commonly encountered in revision surgery and are often due to mechanical abrasion, osteolysis, extraction technique or infection. Boney deficits can be accommodated with cement, bulk support allografts for larger defects or modular revision implants. When encountered these knees should be supported with medullary stem extensions, which assist with load sharing. Most revision implants are cemented at the weak metaphyseal interfaces attached to a noncemented press fit stem extension. It is essential that the intra-medullary stem be inserted centrally in the medullary canal, which may or may not conform to the center of the cut tibial or femoral surface. If there is a discrepancy between central medullary rod position and an optimally positioned joint surface, the difference should be made up with augmentation wedges. In such cases the tibial or femoral surface may have to be recut to conform to the wedges.
Cavitary bone defects are defined as contained (an intact rim of cortical bone surrounding the deficient area) or uncontained (more peripheral location with lack of a bony cortical rim) Disadvantages of allograft include the fact that the surrounding tissues are often damaged with an attenuated blood supply and therefore limiting the ability of the graft to heal and incorporate into the nascent bone. Additionally, allografts can easily become infected from minor wound drainage. Once the allograft is colonized, bacterial eradication is virtually impossible without debridement because the allograft is a dead porous structure where bacteria easily hide. Metallic wedge augments have only an outer surface for bacteria to adhere to, but will obviously never be incorporated or remodel into host bone.
Management of Several Types of bone defects
| Small contained defects | Cement |
| Small uncontained defects < 5mm | Cement |
| Large contained defects | Impacted Cancellous bone graft |
| Large uncontained defects | Structural bone graft Metal wedges Blocks Screw augmented cement |
As mentioned in the hip section, revision knee surgery shares the same goals and operative principles of primary surgery in restoring a functional and durable articulation. However, these surgeries are fraught with potential disaster and should be approached thoughtfully.