



There are three types of cev: positional, idiopathic congenital and teratologic.
Positional Clubfoot
The infant’s foot is in equinovarus but does not have a deep posterior or plantar medial crease and is thought to be the result of intrauterine positioning of the foot. The foot can be passively brought to a plantigrade position and is amenable to cast correction. In general, 1 – 3 months of above-knee cast correction precludes surgical correction.
Idiopathic Congenital Clubfoot
The etiology of idiopathic clubfoot is unknown and occurs in 1 out of 1,000 live births. Males are twice as likely as females to be affected. Initial treatment (birth to 6 months) is manipulation and cast correction. The Iowa (Ponseti) casting protocol is typically used. First, the cavus is corrected by supination of the forefoot and dorsiflexion of the first metatarsal. The supinated forefoot is then abducted under the talus to an outwardly rotated position. The lateral aspect of the talar head is the fulcrum, rather than the calcaneal cuboid joint as in the Kite casting protocol. The calcaneus abducts by rotating under the talus. Once the foot is abducted under the talus to 60º outward rotation, dorsiflexion is attempted.
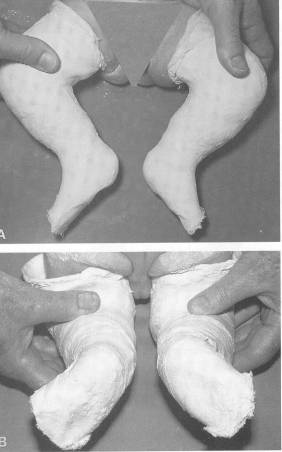
These corrections take 6 to 8 weeks to attain. If the equinus is rigid, a percutaneous Achilles tendon lengthening is done in clinic, or as outpatient surgery with possible inclusion of a posterior capsular release.
Following the conclusion of cast use, a Denis-Browne bar is worn at night for up to 3 years.

The concept of correction with the forefoot supinated is constant, however. Proponents have observed that the rate of full posteromedial release has steadily decreases with experience and now falls under 10%, although up to 40% may require anterior tibialis tendon transfer for residual forefoot supination. The long-term outcome at skeletal maturity has been marked by the excellent appearance and, most importantly, suppleness of the foot.
If correction is not attained by casting techniques with or without Achilles tenotomy, a full or partial posteromedial release (PMR) is undertaken. A PMR may also be required if the onset of treatment is not until after age 8 months, making Ponseti casting extremely difficult if not impossible.
The outcome of surgery is best when performed after 6 months but before 1 year of age. Through a Cincinnati incision, the Achilles, posterior tibialis, and if necessary, long toe flexor tendons are lengthened. Capsular releases include posterior ankle, talonavicular, subtalar, and posterolateral tethers of the calcaneus, and sometimes the calcaneocuboid joint. The more rigid and severe the deformity, the more complete the release must be, although the can increase the risk of over-correction. If the talocalcaneal realignment is suboptimal despite complete subtalar release, the calcaneocuboid joint should be opened medially and laterally to enhance correction. In all studies, the rate of recurrent deformity requiring subsequent surgical intervention (anterior tibial tendon transfer) usually is between 13% and 30%.
Long-term studies show that the surgically treated foot is 1 to 1.5 cm shorter than the contralateral foot and has a smaller calf circumference. The gastrocnemius-soleus complex is only 80% as strong as that of the contralateral foot, with a 23% decrease in the plantar flexion strength. Ankle motion is decreased in 94% of surgically treated feet; ankle valgus is present in two thirds and may compensate for an undercorrected hindfoot or add to the deformity of an overcorrected one. The most common residual effects of surgical intervention are stiffness, forefoot adduction, and supination/cavus.
Teratologic Clubfoot
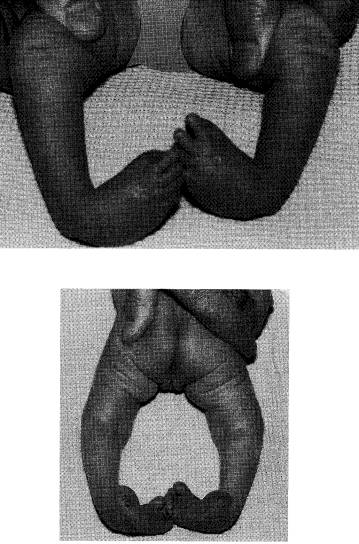
The most common causes of a teratologic clubfoot are either neuromuscular, such as in spina bifida, or syndromic, as in arthrogryposis (see above) or osteochondrodysplasias such as diastrophic dwarfism. The teratologic clubfoot is unlike the idiopathic clubfoot in that attempts at cast correction are more often unsuccessful, making surgery necessary. In patients with spina bifida, the equinovarus deformity is often present at birth and can progress over time. Radical posteromedial release (tenotomy rather than tendon lengthening) provides good results in 76% of cases. Often the anterior tibialis tendon is also lengthened . After radical release, it is essential that not only the talonavicular, but the subtalar joint be pinned in adequate position. The higher the spina bifida lesion, the worse the prognosis. Talectomy can be considered for patients with recurrence of symptoms after radical posteromedial release, and is often done in patients with high-level spina bifida lesions because of a 50% recurrence rate after soft-tissue surgery alone.
For the rigid teratologic clubfoot resulting from arthrogryposis or osteochondrodysplasia, initial casting is done prior to surgery. A radical soft-tissue release of the Achilles tendon, posterior tibialis and flexors, and capsular releases are required. These joints, narrowed by disuse and paralysis, are often difficult to identify. Many authors suggest primary talectomy and often cuboidectomy. Orthotic devices are required to maintain the position postoperatively. In patients in whom symptoms recur after soft-tissue release, talectomy appears to be the best salvage procedure, with better outcome and less complications than triple arthrodesis. In addition, talectomy is useful in a younger age group when a plantigrade foot is essential, but bone maturity precludes triple arthrodesis.
Conclusion
Clubfoot treatment has undergone something of a revolution in the past 10 yrs. With the now world wide recognition of the power of Ponseti casting, the incidence of posteromedial releases has plummeted to under 20% of all children in whom casting is initiated within the first two months of life. Even in teratologic feet, poseti casting has proven to decrease the incidence of or at least the magnitude of surgical intervention. The ponseti method is now being taught the world over, na dis making great impact on the quality of life of children especially in third world nations where surgical intervention is often impossible to attain. Ignacio Ponseti is truly a champion of pediatric orthopedics: now nearing his 90th birthday, he still is teaching his methods in Iowa to eager students from around the world.