

Abnormalities in carpal bone relationships were noted on radiographs obtained in the early 1900s. Subsequent reports focused on the so-called rotational instability of the carpal scaphoid until attention was drawn to the subject in 1972. Describing posttraumatic loss of alignment of the carpal bones, carpal instability patterns have been grouped into four types:
(1) dorsiflexion instability,
(2) palmar-flexion instability,
(3) ulnar translocation, and
(4) dorsal subluxation.
Instability in the carpus has been considered to be static if the radiographic intercarpal relationships do not change with motion, and dynamic if the intercarpal relationships change with manipulation and motion. Radiographic evaluation of the proximal carpal row in the lateral projection in which the radius, lunate, capitate, and third metacarpal should have colinear axes within an approximately 15-degree tolerance. On this projection, the wrist-collapse patterns include:
(1) those in which the distal articular surface of the lunate is tilted to face dorsally, known as a dorsal intercalated segment instability (DISI) pattern, and
(2) those in which the distal articular surface of the lunate faces toward the palm, the volar intercalated segment instability (VISI) pattern.
Dorsal Intercalated Segment Instability (DISI)
When the lunate is rotated dorsally and the scapholunate angle is greater than 70º
This is a description of the deformity but does not describe the pathological process
Causes: SLL injury, scaphoid fracture, Keinboch’s and perilunate injury
End result may be SLAC wrist
Volar Intercalated Segment Instability (VISI)
volar flexion of the lunate relative to the longitudinal
axis of the radius and capitate, when the wrist rests in a neutral position
lunate will tend to flex when there is loss of ulnar support from the triquetrum
may result from disruption of radial carpal ligaments on ulnar side of wrist
characterized by scapholunate angle < 30 deg
usually associated w/ TL dissociation or triquetral-hamate instability;
INSTABILITY CLASSIFICATION
Classification of carpal instability has evolved over the past 20 years. The classification in the table below represents a recent proposal of Dobyns and Cooney. Emphasis is on the location, severity, and radiographic pattern of injury. Prior contributions of Vaughn-Jackson, Fisk, Lichtman, Taleisnik, and others who have identified the important anatomical, mechanical, and kinematic aspects of carpal instability are recognized.
TABLE 66-1 — Carpal Instability—Mayo Classification
Type, Site, and Name
Radiographic Pattern
I. CID
1.1 Proximal carpal row CID
a. Unstable scaphoid fracture
DISI
b. Scapholunate dissociation
DISI
c. Lunotriquetral dissociation
VISI
1.2 Distal carpal row CID
a. AR disruption
RT
PT
b. AU disruption
UT
PT
c. Combined AR and AU disruption
1.3 Combined proximal and distal CID
II. CIND
2.1 Radiocarpal CIND
a. Palmar ligament rupture
DISI, UT of entire proximal carpal row
UT with increased SL space; PT (actually is a CIC)
b. Dorsal ligament rupture
VISI, DT
c. After “radius malunion,” Madelung’s deformity, scaphoid malunion, lunate malunion (see “Adaptive carpus” below)
2.2 Midcarpal CIND
a. Ulnar MCI from palmar ligament damage
VISI
b. Radial MCI from palmar ligament damage
VISI
c. Combined UMCI and RMCI, palmar ligament
VISI
d. MCI from dorsal ligament damage
DISI
2.3 Combined radiocarpal-midcarpal CIND
a. CLIP
VISI, DISI, alternating
b. Disruption of radial and central ligaments
UT with or without VISI or DISI
III. CIC
a. Perilunate with radiocarpal instability
DISI and UT
b. Perilunate with axial instability
AxUI and UT
c. Radiocarpal with axial instability
AxRI and UT
d. Scapholunate dissociation with UT
DISI and UT
IV. “Adaptive carpus”
a. Malposition of carpus with distal radius malunion
DISI or DT
b. Malposition of carpus with scaphoid nonunion
DISI
c. Malposition of carpus with lunate malunion
DISI or VISI
d. Malposition of carpus with Madelung’s deformity
UT, DISI, PT
From Dobyns JH, Cooney WP: Classification of carpal instability, In Cooney WP, Linscheid RL, Dobyns JH, eds: The wrist, St Louis, 1998, Mosby.
AR, Axial radial; AU, axial ulnar; AxRI, axial radial instability; AxUI, axial ulnar instability; CIC, carpal instability combined or complex (dissociative and nondissociative); CID, carpal instability dissociative; CIND, carpal instability nondissociative; CLIP, capitolunate instability pattern; DISI, dorsal intercalated segment instability; DT, dorsal translation; MCI, midcarpal instability; PT, proximal translation; RMCI, radial midcarpal instability; RT, radial translation; SL, scapholunate; UMCI, ulnar midcarpal instability; UT, ulnar translation, VISI, volar intercalated segment instability.
PROGRESSIVE PERILUNAR INSTABILITY
There have been four stages described of progressive disruption of ligament attachments and anatomical relations to the lunate resulting from forced wrist hyperextension.
stage I, scapholunate failure;
stage II, capitolunate failure;
stage III, triquetrolunate failure; and
stage IV, dorsal radiocarpal ligament failure, allowing lunate dislocation.
Rotary Subluxation of Scaphoid
Injuries to the dorsal and volar portions of the scapholunate interosseous ligament, the long radiolunate ligament, and the radioscaphocapitate ligament allow the proximal pole of the scaphoid to rotate dorsally. The scaphoid assumes a more vertical orientation, and eventually the scaphoid separates from the lunate (scapholunate dissociation). Watson and Black observed that rotary subluxation of the scaphoid may present in four types: (1) dynamic, (2) static, (3) with degenerative arthritis, and (4) secondary to a condition such as Kienböck osteochondrosis.
Although a patient may not recall the specific injury, a fall on the extended wrist is the usual cause. The severity of the initial injury may not be appreciated, leading to the mistaken diagnosis of an uncomplicated wrist sprain. Other causes include fracture-dislocations of the wrist, rheumatoid arthritis, and degenerative changes in the ligaments. Typically, patients report pain with activity followed by aching. On examination, pain and tenderness are present along the dorsal radiocarpal articulation at the scapholunate area. Edema may be present with limitation of motion, particularly in flexion.
The following maneuvers are considered to be helpful in evaluating rotary instability of the scaphoid:
The “scaphoid test” in which the examiner places four fingers on the dorsum of the radius with the thumb on the scaphoid tuberosity, using the right hand for the right wrist and the left hand for the left wrist. Ulnar deviation of the wrist aligns the scaphoid with the long axis of the forearm. Applying thumb pressure to the scaphoid tuberosity, the wrist is returned to radial deviation, maintaining the thumb pressure on the scaphoid tuberosity. If the scaphoid is sufficiently unstable, the proximal pole is driven dorsally and pain results.
The “catch-up clunk”: As the wrist under load progresses from radial deviation to ulnar deviation, the scaphoid normally moves smoothly into extension, aligning with the forearm axis. If scaphoid rotary subluxation is present, the lunate remains in a volar-flexed and dorsal position until sufficient pressure is applied so that it suddenly shifts from the volar-flexed position and “catches up” with the scaphoid with a “clunking” sensation.
Although dynamic rotary subluxation of the scaphoid usually cannot be shown radiographically, the diagnosis of static rotary subluxation of the scaphoid can be made on an anteroposterior radiographic view when a gap of more than 2 mm is noted between the scaphoid and the lunate bones. This gap is seen to increase with an anteroposterior view taken with the fist clenched. Other findings on the anteroposterior view include apparent shortening of the scaphoid and the so-called cortical ring appearance of the axial projection of the scaphoid. A separation of 2 mm at the scapholunate articulation is not always symptomatic. The affected wrist should be compared with the opposite normal wrist. The lateral view of the wrist shows the more vertical orientation of the rotated scaphoid.
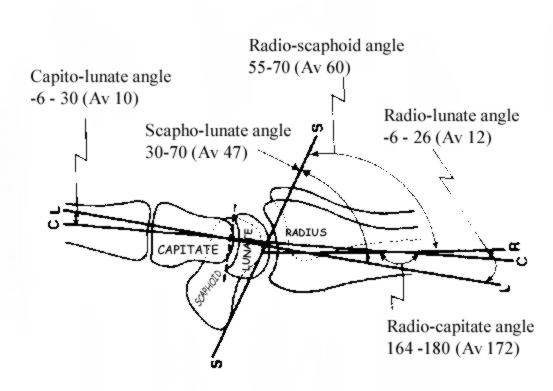
The normal scapholunate angle is 30 to 60 degrees (mean, 47 degrees), and the normal capitolunate angle is less than 20 degrees. The scaphoid rotation leads to the development of the dorsal intercalated segment instability (DISI), in which the scapholunate angle is more than 60 degrees and the capitolunate angle is more than 20 degrees. Occasionally the capitate migrates proximally into the gap created by the separation of the scaphoid and lunate, especially when an axial force is exerted on the capitate, as when making a fist. Degenerative arthritic changes may eventually develop.
Closed treatment for the acute rotary subluxation of the scaphoid consists of attempting reduction by placing the wrist in neutral flexion and a few degrees of ulnar deviation. Percutaneous pinning with one Kirschner wire placed through the scaphoid into the capitate and a second through the scaphoid into the lunate has been described. If closed reduction is unsuccessful, arthroscopic reduction and percutaneous pin fixation can be attempted; however, open reduction through a dorsal approach with closure of the scapholunate gap, Kirschner wire internal fixation of the lunate to the scaphoid, and ligament repair usually are indicated. Management of an old rotary subluxation of the scaphoid may require reconstruction of the scapholunate interosseous ligament with a segment of the extensor carpi radialis brevis tendon plus Kirschner wire fixation after the graft has been passed through the scaphoid into the adjoining lunate. Insufficient experience with this procedure has been reported in the literature to provide data for comparing results with nontreatment.
Anterior Dislocation of Lunate
The most common carpal dislocation is anterior dislocation of the lunate. On a lateral radiographic view of the normal wrist, the half-moon-shaped profile of the lunate articulates with the cup of the distal radius proximally and with the rounded proximal capitate distally. On an anteroposterior view the normal rectangular profile of the lunate when dislocated becomes triangular because of its tilt. An anteriorly dislocated lunate can cause acute compression of the median nerve, which if prolonged can result in a permanent palsy. If a patient’s condition permits and if swelling is not excessive, the lunate bone should be reduced promptly. Because an open release of the transverse carpal ligament may be required, every effort should be made to reduce and control the swelling to permit wound closure. When the injury is treated early, manipulative reduction usually is possible, and immobilization for 3 weeks with the wrist in slight flexion is required. When treated after 3 weeks, the injury can be difficult to reduce by manipulation, and open reduction may be necessary. When the lunate cannot be reduced by open reduction, a reconstructive procedure such as proximal row carpectomy or arthrodesis may be necessary.
Palmar Transscaphoid Perilunar Dislocations
Palmar transscaphoid perilunar dislocations are extremely rare. The mechanism of injury as a fall on the dorsum of the flexed wrist. This is directly opposite to the mechanism that produces a dorsal perilunar dislocation. In their patient, reduction was early, and the fracture was found to be stable with the wrist in dorsiflexion but unstable in flexion.
Dorsal Transscaphoid Perilunar Dislocations
Like the isolated scaphoid fracture, diagnosis of this injury may be overlooked and delayed. It can be associated with other injuries of the upper extremity. Early reduction by closed manipulation is best. When accurate reduction of the scaphoid fracture is not obtained, open reduction, internal fixation, and, when indicated, bone grafting may be necessary.
Closed reduction may be possible up to 3 weeks after injury. Many of these injuries later require open reduction, and internal fixation with Kirschner wires may be necessary for stability. Although Boyes reported successful open reduction as late as 6 weeks after injury, after 2 months, open reduction may not be possible. Proximal row carpectomy or arthrodesis of the wrist may be indicated.
Triquetrolunate and Midcarpal Instabilities
Axial loading of the hyperextended pronated wrist contributes to injury of the ligamentous supports of the triquetrolunate and midcarpal joints. Disruption of the triquetrolunate, dorsal intercarpal, and radiotriquetral ligaments leads to laxity on the ulnar side of the wrist. When examining the wrist for triquetrolunate and midcarpal instability, Lichtman and Martin reported the following findings. Patients with triquetrolunate instability usually report pain on the ulnar aspect of the wrist, with or without an associated wrist click in radial and ulnar deviation. Usually a traumatic event could be described. The physical examination usually reveals tenderness over the ulnar aspect of the wrist in the region of the triquetrolunate joint and a click usually can be reproduced in radial and ulnar deviation. According to Reagan, Linscheid, and Dobyns, ballottement of the lunotriquetral joint can help in diagnosing this instability. The lunate is stabilized with the thumb and index finger of one hand, and an attempt is made to displace the triquetrum and pisiform dorsally and palmarward with the opposite hand. Usually, excessive laxity, pain, and crepitance constitute a positive test. If the triquetrolunate injury is a tear or sprain, the usual static radiographs are normal. If there is triquetrolunate dissociation, the triquetrum may be displaced proximally on the anteroposterior view. This may be exaggerated with ulnar deviation, creating overlapping of the lunate and triquetrum. Although arthrography can be helpful in evaluating triquetrolunate ligament injuries, arthroscopic examination usually is diagnostic.
Palmar instability in the midcarpal region (capitolunate) is thought by Lichtman et al. to be a manifestation of laxity of the ulnar arm of the arcuate ligament. This laxity allows the proximal carpal row to develop a palmar-flexed position (volar intercalated segment instability [VISI]). The works of Horii et al. and Ritt et al. indicate that defects in the dorsal intercarpal and radiotriquetral ligaments contribute to static malpositioning. Most patients have the sensation of a painful “clunk” with ulnar deviation and pronation of the wrist. A palmar sag can be identified at the level of the midcarpal joint on physical examination. The clunk can be reproduced by passively moving the hand from the relaxed neutral position into ulnar deviation. As the wrist reaches its extreme of ulnar deviation, a palpable sensation or a “clunk” is noted. At this time the volar sag will be corrected. The radiographic examination usually reveals a VISI pattern. With the wrist in neutral position and unsupported, the scapholunate angle decreases to less than 30 degrees in the lateral projection. Video fluoroscopy or cineradiography can be helpful in assessing wrist instability.
OTHER INSTABILITY PATTERNS
Other instability patterns have been described and may require treatment. They include dorsal instability patterns related to malunited fractures of the distal radius or lax ligaments (non-dissociative), capitolunate instability patterns (“CLIP” wrist), volar instability related to laxity in the triquetrohamate ligament, ulnar translocation of the carpus resulting from severe traumatic or inflammatory ( rheumatoid) disruption of the dorsal and volar radiocarpal ligaments, and scapholunate advanced collapse (SLAC). According to Watson and Black, triquetrohamate instability usually is associated with other significant ligament injuries in the wrist. Ulnar translocation of the carpus, usually seen in patients with rheumatoid arthritis, also may be present after major ligament disruptions in the wrist. The SLAC pattern usually is seen after conditions that lead to rotary subluxation of the scaphoid, resulting in loss of cartilage and degenerative changes in the radioscaphoid and capitolunate joints with sparing of the radiolunate joint.