

Overview
Meniscal knee injuries are very common. Historically, the menisci were not felt to be important structures and total menisectomies used to be a common operation performed for meniscal tears. However, we have learned that the menisci play an important role in load transmission, improving joint congruity, and joint stabilization. It is estimated that the menisci carry 30-70% of the total load across the knee.
The menisci are fibrocartilaginous rings found in the medial and lateral joint compartments of the knee. The medial meniscus is C-shaped and the lateral meniscus is more circular. The medial meniscus tends to have more attachments to surrounding structures than the lateral meniscus and is less mobile. Medial meniscus tears are more common than lateral meniscal tears.
Collagen makes up 60-70% of the dry weight of the meniscus with 90% being type I collagen. At birth, the entire meniscus is vascular but by the age of 10 only the outer 10-30% of the peripheral rim is vascular.
History
Meniscal tears can be acute or chronic in nature. Acute meniscal injuries tend to be associated with a twisting or cutting injury. The knee may swell soon after injury. Chronic meniscal tears are more degenerative in nature. Chronic tears tend to occur in the older population and are characterized by recurrent knee swelling and pain. Patients with meniscal injuries may notice a clicking or catching. With larger bucket handle tears involving the majority of the meniscus, patients often complain of knee locking with the inability to fully extend the knee.
Physical Examination
As always, it is important to perform a full physical exam of the knee to rule out other potential injuries. The knee should be inspected and palpated. Patients with meniscal injuries may have swelling and joint line tenderness. There may also be a palpable Baker’s cyst in the posterior knee. In adults, a Baker’s cyst is frequently associated with a meniscal tear. Range of motion should be examined. Patients with locked bucket handle tears will have difficulty fully extending the knee. Posterior horn meniscal pathology may show pain with deep flexion. McMurray’s testing is the classic provocative maneuver for diagnosing a meniscal tear. McMurray’s testing of the lateral meniscus is performed by flexing the knee, externally rotating the foot and applying a valgus load while extending the knee. Testing of the medial meniscus is performed by flexing the knee, internally rotating the foot and applying a varus load while extending the knee. A positive test is elicited pain and/or a palpable joint line click and is suggestive of meniscal pathology.
Imaging
Plain radiographs should be obtained in the work up. An MRI can assist in the evaluation of a meniscal tear although is not necessary if the history and physical exam suggest meniscal pathology. The accuracy of MRI is now considered around 95% in detecting meniscal tears.
Treatment
It is estimated that approximately 40% of patients with pain, swelling, and an exam consistent with a meniscal tear will get better with non-operative measures. If symptoms do not improve within 6-12 weeks, operative management is typically recommended.
The operative management goal of meniscal tears is to preserve as much meniscal tissue either by repairing the meniscal tear or performing a menisectomy back to a stable rim. Studies have shown significant changes in articular contact pressures with meniscal excision. Because the menisci are so important in load transmission, a partial menisectomy should remove the unstable meniscal flap and the amount of excised tissue should be minimized. The decision to repair vs. excise depends on patient age and activity level as well as pattern, age and location of the tear.
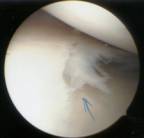
Arthroscopic view: torn meniscus
The outer 10-30% of adult meniscal rims are vascular and receive their blood supply from the geniculate arteries. The inner two-thirds of the meniscal rim are avascular and receive their nutrition from the synovial fluid. This is an important concept in the treatment of meniscal tears. In order for a meniscal repair to heal, it needs an adequate blood supply. Most would support the concept that meniscal repairs should only be attempted in patients with tears in the outer vascular meniscus. The ideal situation for a meniscal repair is the young active patient that sustains a large, acute bucket handle tear of the outer rim. There are numerous described surgical techniques for meniscal repair.
The load transmission properties of the menisci are important in preserving the cartilage surfaces and meniscal deficient knees are prone to future degenerative changes. Some large peripheral meniscal tears are not repairable. Meniscal allograft transplantation is an option in select meniscal deficient knees although long term results at this point are unknown.